Piano Lessons, Scaramuzza Technique
Piano Finger Technique (London): The Anatomy of Touch, Finger Independence, and Efficient Motion

Mar
Piano Finger Technique Complete Analysis
Piano Finger Technique — Anatomy of Touch, Independence & Efficient Motion (London)

Why precise finger technique matters
There is a persistent myth that piano finger technique is mainly a question of willpower: lift higher, strike harder, practise longer. The reality is less heroic and more useful. What we call “technique” is, in large part, the management of joints, tendons and coordinated muscle action so that sound is produced with the least avoidable effort.
When that coordination is working, the results are immediate: cleaner passagework, a wider dynamic range, and endurance that feels almost unremarkable. When it fails, the symptoms are equally familiar—stiff wrists, collapsing knuckles, a thumb that seems to do far too much, and the nagging discomfort that musicians euphemistically label “a bit of tightness”.
This guide sets out the underlying hand mechanics of piano playing—bones, joints, tendons, and the motor-control principles that govern them—then connects that anatomy to efficient movement, including Scaramuzza’s five-movement framework. Along the way, we’ll look at common technical faults teachers recognise quickly, how bench and keyboard setup influence strain, and when pain should prompt a referral to a performing-arts physiotherapist rather than another week of “pushing through”.
Technique is load-management. When joints, tendons and timing cooperate, sound improves while effort quietly disappears—often the most reliable sign you’re moving efficiently.
The anatomy of the pianist’s hand — bones, joints, tendons & control
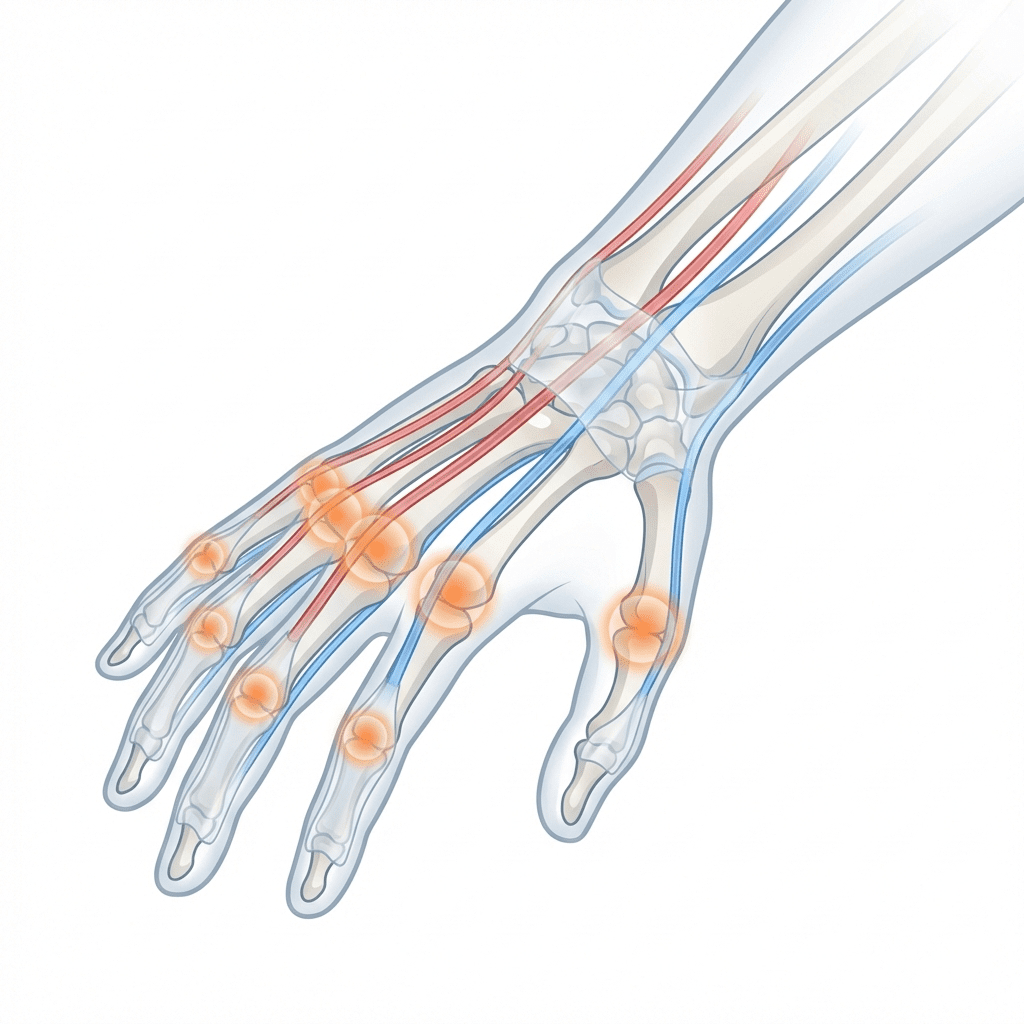
Fingers: bones and joints that actually do the work
The finger mechanism is built from metacarpals and phalanges, connected by three main joint levels: the MCP joints (metacarpophalangeal, at the knuckles), the PIP joints (proximal interphalangeal), and the DIP joints (distal interphalangeal, near the fingertip). These joints don’t operate in isolation; they are stabilised moment-to-moment by muscle activity both in the forearm and within the hand.
Tendons and the forearm “engine”: flexors, extensors, and sheaths
Most of the heavy lifting is done by extrinsic muscles in the forearm. The flexor digitorum superficialis and flexor digitorum profundus flex the fingers; the extensor digitorum extends them. Their tendons travel through tight tendon sheaths and pulleys across the wrist and palm—efficient for force transmission, but not especially forgiving when friction and overload accumulate.
Intrinsic muscles: independence, stability, and the “hidden” coordination layer
Inside the hand itself, lumbricals and interossei help stabilise joints and support finger independence. The lumbricals, arising from the flexor tendons, can flex the MCP joints while extending the PIP and DIP joints, coordinating flexor and extensor systems in one balanced action. This is part of why a poised hand can feel both firm and mobile—an architectural steadiness rather than a muscular clamp.
Wrist: a flexible hinge, not a fixed bracket
The wrist is often treated as an aesthetic detail, yet it is a central load-management point. A broadly neutral wrist—neither strongly flexed nor extended—helps distribute force and reduces stress on tendons. Side-to-side angles matter too. Ulnar deviation (hand bent toward the little finger) and radial deviation (toward the thumb) happen naturally during playing, but excessive deviation increases strain. An ulnar-angled hand may overload the extensor carpi ulnaris tendon on the little-finger side; a strongly radial angle stresses the thumb side. Bench and keyboard alignment are not “posture trivia”; they are among the simplest ways to reduce unnecessary deviation.
Motion types & economy of motion — Scaramuzza’s five movements
Pianistic motion looks complex because it is layered. Yet one of the virtues of the Scaramuzza tradition is its clarity: it describes five primary movement categories—finger, wrist, forearm, arm (shoulder), and rotation—that can account for most playing actions. In performance they blend, but in learning and diagnosis it helps to separate them.

1) Finger movement
Finger movement is the local flexion and extension at the MCP and interphalangeal joints. It is indispensable for rapid scales, light passagework, and fine dynamic control. Scaramuzza teaching often stresses that fingers should “roam freely” with minimal help from larger muscle groups—meaning, in practice, that the finger mechanism is not bullied by a fixed wrist or tense forearm.
2) Wrist movement
Wrist movement includes short bending and subtle rotational actions. A supple wrist can provide release in staccato, trills, accents, and levelling motions that keep the hand aligned across changing terrain. In Scaramuzza-based instruction, wrist tension is minimised and wrist actions are used with discretion—often to facilitate speed—rather than as a substitute for sound arm-weight coordination.
3) Forearm movement (the “chord movement”)
Forearm dropping and lifting transfers weight from shoulder through forearm into the key. Scaramuzza describes a chord action in which elbow and forearm rise (with the wrist) and then the weight drops smoothly for a full tone. This is not theatrical; it is economical. It aims to use gravity and body weight rather than concentrated finger force—particularly helpful for repeated chords and rich sonority.
Instrument design plays a role. On a grand piano, the horizontal action can make gravity-assisted weight transfer feel natural; on an upright, where springs contribute more to key return, players may feel they must “do more” with the fingers. The risk is that “more” becomes gripping. The better solution is usually a modest technical adaptation—still weight-informed, still joint-friendly—rather than a wholesale turn toward muscular effort.
4) Arm movement (from the shoulder)
Arm movement involves the larger release of the whole arm from the shoulder, often used at the start of phrases or when approaching large dynamic changes. The arm is raised and dropped freely onto the keys with relaxed musculature. Done well, it is a way of preparing sound without recruiting the smaller structures—fingers and wrist—as the first line of defence.
5) Rotational movement
Rotation is the turning of the forearm (pronation and supination), subtly reorienting the hand for leaps, repeated patterns, or uneven key groupings without twisting the wrist or hiking the shoulder. Scaramuzza teaching sometimes uses the idea of a pivot finger (often the thumb) while the wrist follows the rotational pathway. This can make transitions smoother and tone more even, especially when the hand must negotiate black keys without contortion.
Finger function and coordination — independence, interdependence, and control
Healthy piano finger technique is not a contest of isolation. It is closer to chamber music: different parts acting independently when needed, but always in negotiation with the whole.
Co-contraction: useful stability, harmful rigidity
One central concept is co-contraction: the simultaneous activation of opposing muscle groups, such as finger flexors and extensors, to stabilise a joint. A low baseline level is normal and helpful. Research described in a recent scoping review notes that during finger flexion, extensors also engage slightly, effectively bracing the joint for control. The same review also highlights the darker side: excessive co-contraction increases stiffness and fatigue, and can raise injury risk by turning adaptability into rigidity.
Individuation: why “independent fingers” are never fully independent
Teachers talk about finger independence, but anatomically it is constrained. Some fingers share muscle bellies and tendon connections; extensor structures interlink. This is why the ring and little finger can feel like reluctant partners. Better coordination often comes not from forcing separation, but from reducing unnecessary tension—especially in the palm—so that the intrinsic muscles can stabilise without clamping.
Active versus passive motion: using weight rather than over-lift
Another practical distinction is active versus passive motion. Players often overuse active finger lifting—high finger extension between notes—particularly when chasing volume. But downward key motion can often be supported by passive elements: gravity, arm weight, and efficient transfer through a neutral wrist. Keeping finger lift to the minimum needed for clarity can reduce joint torque and spare the tendon sheaths from needless friction.
Common mechanical faults — what teachers notice first
Most playing-related problems announce themselves in a few repeatable patterns. A skilled teacher watches for them not to criticise, but to locate where load is being mismanaged.
Stiff, raised shoulders or elbows
A “hung” posture shifts work to neck and shoulder muscles and often accompanies breath-holding. A calmer shoulder line, with elbows slightly forward, tends to support better weight transfer and reduces the temptation to grip through the forearm.
Bent wrists or collapsed knuckles
A strongly flexed wrist increases tension in the finger flexor tendons; an excessively extended wrist or collapsed knuckles can flatten the finger structure and strain extensor pathways while weakening control. The practical target is usually a neutral to slightly extended wrist with knuckles forming a gentle curve—stable, but not rigid.
Ulnar deviation on strong chords
If the hand consistently drifts toward the little-finger side under force, tendons can be compressed and overloaded. This often improves with simple alignment changes: bench position, shoulder squareness, and allowing the elbow to sit more naturally above the keys rather than behind them.
Tense forearms and “overgripping”
Clenching, over-fixing the wrist, or repeated flicking actions can contribute to tendon irritation, including tenosynovitis. A sobering diagnostic clue is pain during very soft playing: if even quiet notes produce soreness, something is being loaded unnecessarily. Playing through it rarely improves the situation.
Overlifted fingers (“flapping”)
High finger lifts between notes tend to recruit the extrinsic extensors more than necessary. The visual signature is chatter: fingers rising theatrically, arriving late, then compensating with extra force. A calmer, closer-to-the-keys approach often supports both speed and ease.
Dominant thumb posture
The thumb’s carpometacarpal joint and thenar muscles take substantial load during crossings. A rigid thumb or one that collapses can stress ligaments and contribute to tendon-sheath irritation. The more sustainable aim is a thumb that flexes from the palm rather than jamming sideways into the key.
Seat and bench problems (often the root cause)
Technical faults are sometimes just ergonomics in disguise. If a bench is too low, a player may hunch or raise shoulders; too high, and wrists may hyperextend or the body may slump for balance. One physiotherapist writing on musicians’ PRMD notes that typical practice seating often fails to accommodate different body shapes. In studio terms, a reasonable starting point is adjusting height until forearms are roughly level with the keys, with elbows slightly above, so the wrist can remain neutral and weight transfer can function.

When to stop and refer: persistent numbness, shooting pain, swelling, catching at the thumb tendon (often discussed in relation to De Quervain’s syndrome), or any loss of normal finger movement should prompt medical evaluation. If a finger cannot bend or straighten, if swelling is rapid, or pain is severe at rest, treat it as urgent rather than “a technique issue”.
Adjusting technique for repertoire and context
Repertoire exposes mechanics. Large stretches in Brahms or Rachmaninoff can strain smaller hands if the wrist is held immobile; redistribution, alternative fingerings, and rotational assistance can reduce load. Repeated notes, octave passages and trills can overload a single tendon line; alternation and grouping are common musical solutions that also happen to be physiological ones.
Instrument matters too. On a grand, weight technique can feel efficient because gravity can help key return; on an upright, the action may feel heavier and spring-driven, tempting players to lean into the wrist. Teachers often tailor advice accordingly—without abandoning the central principle: force should be distributed through coordinated movement rather than concentrated in one small structure.
If a passage remains provocative even after adjustments, the most professional choice can be temporary modification: simplify an ornament, drop a note in a dense texture, or schedule practice so the hardest material is interleaved with easier work and genuine breaks. This is not surrender; it is load management.
Seeking help in London — clinics, referrals, and sensible escalation
London has unusually strong resources for musicians when playing-related pain becomes persistent. The British Association for Performing Arts Medicine (BAPAM) maintains a directory of clinicians familiar with musicians’ demands and runs clinics in central London. The Institute of Sport, Exercise and Health (ISEH) at UCL collaborates with BAPAM and conservatoires, bringing sports-rehab expertise into performing-arts contexts. Chartered physiotherapists with performing-arts training—often accessible via BAPAM—can assess tendon and nerve issues with the specificity pianists need.
A GP may refer onward to orthopaedics or hand therapy if tendon or nerve injury is suspected. The more general point is simple: early assessment is usually cheaper than prolonged self-diagnosis. Musculoskeletal problems are common across musicians’ careers, and delay tends to turn manageable irritation into a longer rehabilitation story.
Finally, workload and psychology are not footnotes. Research on student pianists with chronic pain notes the role of internal pressure and inadequate support, and recommends a biopsychosocial approach—technique, schedule, and stress addressed together. If you notice pain correlating with anxiety, fatigue, or relentless practice blocks, it is worth treating that as information, not weakness.
Evidence, references & further reading
This article draws on performing-arts medicine writing on playing-related musculoskeletal disorders, recent research on co-contraction and motor control in pianists, and published discussions of Scaramuzza-based technique. The aim is not to medicalise music-making, but to describe the mechanism honestly enough that teachers and players can make better decisions—especially when discomfort begins to colour practice.
Frequently asked questions on Piano Finger Technique
What causes tendons and fingers to hurt when playing?
Overuse and inefficient mechanics can irritate tendon sheaths and contribute to tendinitis or tenosynovitis. Common drivers include poor wrist posture (excess flexion/extension), excessive ulnar or radial deviation, and long sessions without breaks. Thumb-heavy patterns can also contribute to De Quervain’s-type symptoms.
How do I improve finger independence without forcing it?
Start by reducing global tension: shoulders, forearms, and palm. Anatomical interconnections limit true isolation, so the goal is clearer individuation rather than “perfect independence”. Scaramuzza-based cues often focus on free finger motion supported by weight transfer, not by gripping.
What is co-contraction, and is it bad?
Co-contraction is the simultaneous activation of opposing muscles to stabilise joints. A small amount supports control; excessive co-contraction increases stiffness and fatigue and may raise injury risk. The practical sign is a hand that feels braced even during easy playing.
Does bench height really affect piano finger technique?
Yes. Too low can provoke hunching and raised shoulders; too high can lead to wrist hyperextension or slumping for balance. A useful starting point is forearms roughly level with the keys and elbows slightly above, allowing a neutral wrist and natural weight transfer.
Grand vs upright: should my technique change?
The principles stay the same, but the feel differs. Grand actions can favour gravity-assisted weight transfer; uprights may feel more spring-driven, tempting extra finger effort. The aim is to adapt without gripping—keeping joints mobile and load distributed.
When should I see a specialist?
Seek help for persistent pain, numbness, tingling, swelling, catching at a tendon, or any impairment of finger movement. In London, performing-arts medicine pathways through BAPAM and related clinics can provide musician-specific assessment and referral.
Next step: a technique assessment that respects the body
If your piano finger technique feels inconsistent—or if discomfort is beginning to shape your repertoire choices—it is worth having it assessed with the same seriousness you would give tone, rhythm, or pedalling. At WKMT London, Scaramuzza-trained piano tutors work with players to reduce unnecessary tension, improve weight transfer, and diagnose mechanical habits that invite strain.
To continue, explore WKMT London for lessons and consultations, or speak to a tutor about whether a playing-related health referral is appropriate alongside technical work.
Notes & attribution
This article is educational and does not replace medical diagnosis. If symptoms are severe, sudden, or neurological (numbness/tingling), consult a qualified clinician.
Sources
Rezzuto J., “What Is The Scaramuzza Technique And Why Is It Powerful?”, Music Matters Blog (2021)
Wang Y., Occupational Diseases and Countermeasures of Pianists, Health 11(9):1147–1151 (2019)
Institute of Sport, Exercise & Health (London), Performing Arts Medicine MSc (info)